
(pdf)
The Republican and Democratic parties have each released some version of a platform or agenda for the 2020 election, and the release of these platforms raises several important questions for taxpayers.
Health care is, yet again, one of the most important issues facing policymakers this election season. National Taxpayers Union (NTU) has a stake in federal and state health policy for several reasons, chief among them that good health policy can foster innovation for consumers and cost savings to major federal- and state-run health programs for taxpayers.
What follows is an analysis of the 2020 Democratic Party platform on health care and the 2020 Trump campaign second-term agenda on health care (the Republican Party declined to produce a comprehensive platform this year). We will follow up with some NTU suggestions for pro-growth, pro-taxpayer alternatives that could serve either party well in 2021 and beyond.
Comparison
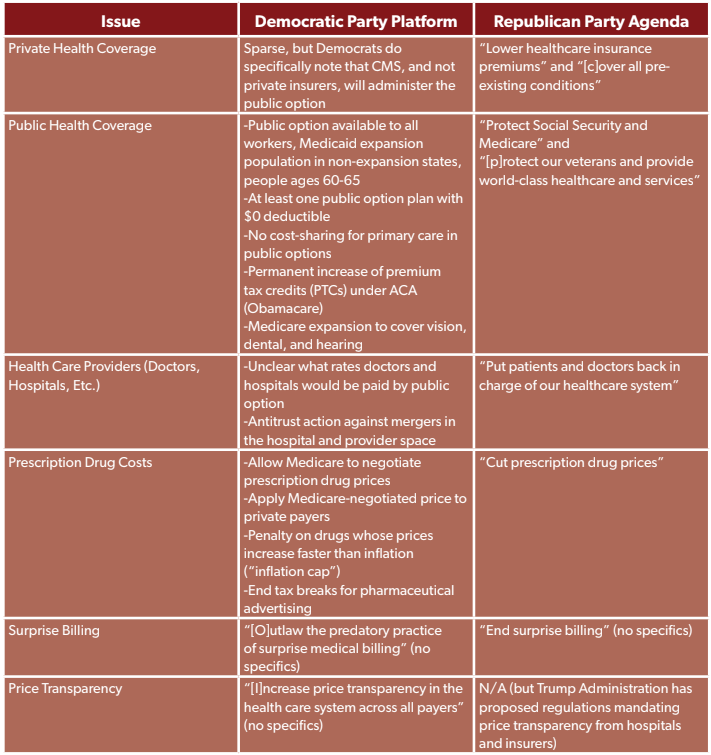
While a detailed analysis of the two party platforms follows, it may be helpful to quickly and visually compare how Republicans and Democrats propose to tackle a variety of health policy issues. Illustrated in the chart below:
The Democratic Party Platform
Democrats held their convention first this year, and published their platform at that time as well. The central plank of the Democratic Party health care platform is the creation of a public option on the Affordable Care Act (ACA, or Obamacare) marketplace, which would compete with private health insurers currently offering plans in marketplaces around the country:
The public option will provide at least one plan choice without deductibles; will be administered by CMS, not private companies; and will cover all primary care without any co-payments and control costs for other treatments by negotiating prices with doctors and hospitals, just like Medicare does on behalf of older people.
Around four million Americans who would otherwise be eligible for Medicaid in the 12 states that have not expanded Medicaid under the ACA would be automatically enrolled in the public option without premiums. Older adults could access the public option or Medicare starting at age 60 (rather than the current Medicare retirement age of 65).
The public option plan as Democrats propose it raises several questions relevant to taxpayers:
Given at least one public option plan “will provide at least one plan choice without deductibles,” how many public option plans do policymakers plan on offering? Will a small set of plans be offered nationally, or will a series of plans be offered with different rates, coverage, and networks based on state or region?
How will policymakers rate premiums in the public option plans? Will they follow the ACA model that limits rating to region, type of plan (individual vs. family), age (3:1), and tobacco use (1.5:1)? Will taxpayers or certain public option enrollees subsidize premiums for the millions of Americans who receive the public option at no cost, and if so what is the impact on premiums?
How will policymakers handle present and future political temptations to offer the public option at a cost-sharing rate (inclusive of premiums, deductibles, copayments, and coinsurance) that is less than the cost of providing the public option to millions of Americans? If policymakers do plan to offer the public option at a price less than the cost of providing care, how do they avoid a situation where private insurers exit the marketplace because they can’t compete with artificially low government prices?
Why do Democrats insist on having CMS administer the public option rather than private companies? (There is no compelling reason listed in their platform.) Would policymakers change their position if and where evidence suggests that private companies can deliver more efficiency and savings for taxpayers, while retaining quality for enrollees?
How will policymakers build effective networks, either on a region-by-region basis or at the national level, while aggressively negotiating prices “just like Medicare”? Studies suggest commercial reimbursement averages between 150 and 225 percent of Medicare prices for inpatient services, 160 and 360 percent for outpatient services, and 118 and 180 percent for professional services. Will policymakers negotiate significant payment cuts for providers and hospitals, risking consolidation and/or reduced provider supply? Or will they pay providers more than Medicare rates, which commits larger allocations of taxpayer dollars to the public option?
How do policymakers avoid adverse selection issues, where only patients with high health care costs sign up for the public option?
More broadly, the platform tries to achieve the difficult balancing act of a nominee who opposes single-payer “Medicare for All” plans with a progressive faction of the party that insists such a policy is a necessity. How the party continues that balancing act if swept into power this fall is a key question with multi-trillion-dollar implications for taxpayers.
The platform includes several additional measures that NTU has opposed in the past, some of which have support from both the left and the right. This includes:
Allowing Medicare to negotiate prescription drug prices, and having that price apply to public and private payers: NTU has noted that the projected savings from prescription drug negotiation are somewhat phantom, unless paired with some kind of negotiating tool for the government. The tool that Speaker Nancy Pelosi (D-CA) recently proposed giving federal bureaucrats was a steep tax on a manufacturer’s gross sales of a drug for refusing a government price, which would impact the availability of future cures and could put small and mid-sized manufacturers out of business. Despite some bipartisan support for Medicare prescription drug negotiation, it should be noted that Part D, Medicare’s prescription drug benefit, already allows manufacturers, private plans, and pharmacy benefit managers (PBMs) to negotiate the price of drugs. This system has delivered low premiums and plentiful plan options to America’s seniors.
Capping prescription drug prices at the rate of inflation: As NTU explained about Part D inflation cap proposals last year, “the larger the difference between this government-imposed cap (on a [Part D] program with 45 million enrollees) and the market price for a drug, the more plan sponsors and drugmakers will seek to recoup those costs elsewhere.” Indeed, setting prices in one program only pushes the cost bubble onto other patients, other treatments in a manufacturer’s product line, or both.
Permanently increasing premium tax credits (PTCs) under the ACA: The platform endorses a provision of legislation that the Democratic House passed and NTU opposed earlier this year, which the Congressional Budget Office (CBO) projected would cost $212 billion over 10 years. This legislation would make the values of PTCs more generous by lowering the share of income that households contribute to their ACA premiums (from 9.5 percent to 8.5 percent). The bill would also make PTCs eligible for households beyond 400 percent of the federal poverty line (FPL), which in 2020 is $104,800 in annual income for a family of four. NTU does not believe that subsidies for six-figure households is the most efficient use of limited taxpayer dollars and, as we have noted before, with the ‘percentage of household income’ standard “[i]t is easy to see how exponential premium growth, compared to more modest wage growth, could lead to exploding federal costs for PTCs, both above and below 400 percent of the FPL.”
Other parts of the Democratic Party platform require more detail. The party claims it will “outlaw the predatory practice of surprise medical billing,” but is silent on how to address inevitable payment disputes between plans and providers. The party says it will “increase price transparency in the health care system across all payers,” but does not point to specific ways it would so (such as the Trump administration’s recent proposed price transparency regulations). The party also threatens antitrust action against a series of health care sectors, including hospitals, insurers, and pharmaceutical manufacturers, but declines to call out specific mergers or acquisitions of concern.
Most importantly, the party declines to share how it will pay for the public option, PTC expansion, and Medicare expansion to cover dental, vision, and hearing, among numerous other health initiatives that will presumably require federal tax dollars. Prescription drug negotiation, an inflation cap, reduced paperwork for medical billing, and the elimination of tax breaks for prescription drug ads alone will not pay for this agenda, and the party owes taxpayers a fuller explanation of the tax-and-spend tradeoffs in their platform.
The Republican Party Platform
Unfortunately, the Republican Party agenda offers few details to work with. The party declined to enact a platform for 2020, kicking that work to 2024, and the Trump campaign’s recently released second-term agenda has seven very generic bullet-point items:
Cut prescription drug prices;
Put patients and doctors back in charge of our healthcare system;
Lower healthcare insurance premiums;
End surprise billing;
Cover all pre-existing conditions;
Protect Social Security and Medicare; and
Protect our veterans and provide world-class healthcare and services.
All seven of the above items read more like goals than policy proposals. Nonetheless, the following questions may be relevant to taxpayers:
If given a second term, will the Trump administration reject prescription drug proposals that could actually raise costs for taxpayers and consumers, like “Buy American” mandates, prescription drug importation from Canada, a "Most Favored Nation" plan for drugs in Medicare Parts B and D, and an inflation cap for Medicare Parts B and D? Will the administration instead pursue productive public-private partnerships like it did with CMS’ insulin model and its negotiations with manufacturers of PCSK9 inhibitors?
What does it mean to “put patients and doctors back in charge of our healthcare system”? At NTU, we hope this means expanding and promoting the use of health savings accounts (HSAs), which empower consumers to have more control over their coverage and serve the broader goal of de-linking health coverage from employment.
How would a Trump administration lower healthcare insurance premiums over the next four years? Though the market structure of Medicare Advantage and Part D has led to stable or even declining premiums over the past several years, and short-term limited duration insurance (STLDI) offers certain consumers a low-cost and temporary alternative to expensive marketplace plans, lowering premiums is a tall order for policymakers - especially in the employer plan market that covers a plurality of Americans. The campaign owes taxpayers a fuller explanation.
How would a second Trump term end surprise billing? The administration has declined to strongly endorse one payment dispute mechanism over the others, but merely opposing surprise billing is no more a policy proposal for the Republicans than it is for the Democrats. NTU encourages both parties to adopt a simpler, less government-heavy solution for surprise billing disputes such as a contract-based model or “truth in advertising” enforcement.
What’s the campaign’s proposal for pre-existing condition protections? The administration supports a complete repeal of the ACA, but the ACA actually includes six overlapping pre-existing condition protections - no coverage exclusions, no premium rating, guaranteed availability of coverage, guaranteed renewability of coverage, no eligibility restrictions, and no excessive waiting periods for coverage. Does the campaign propose doing away with all of these restrictions or some of them? If so, what’s a replacement plan that still “cover[s] all pre-existing conditions?”
While the campaign pledges to “protect Social Security and Medicare,” how will it address the forthcoming trust fund crises in both programs? Democrats have already rejected cost-saving measures like raising the retirement age. Will the Trump campaign’s pledge here block any future efforts to save these programs?
Overall, the Trump campaign’s second-term health care agenda is lacking in details. The campaign and the Republican Party owe consumers and taxpayers fuller explanations. Fortunately, their allies in the Republican Study Committee and elsewhere are offering expansive, detailed platforms for the GOP. NTU also hopes some of the below alternatives can be adopted by one or both parties as they consider a governing agenda for 2021.
A Pro-Taxpayer Platform
The following policy proposals are, in no particular order, among NTU’s most recent and consistent suggestions for policymakers. We believe members of both parties can support elements of this platform, and indeed several of the proposals below have attracted endorsements from both Republicans and Democrats in Congress.
Expand Health Savings Accounts (HSAs): In October, NTU released eight proposals for expanding and promoting the use of HSAs. One, allowing HSA holders to use their account dollars for over-the-counter medications, was enacted as part of the CARES Act. Congress should raise annual contribution limits, allow anyone to open and contribute to an HSA (not just people in a high-deductible health plan), and allow HSA dollars to be spent on health insurance premiums. Recent HSA legislation has attracted the support of some Congressional Democrats, suggesting bipartisan momentum on the broader issue.
Enact pro-growth tax reform that boosts the medical supply chain: NTU believes lawmakers should avoid costly and counterproductive “Buy American” mandates for medical goods, but we have pointed lawmakers to pro-growth alternatives that would support domestic manufacturers while avoiding disruptions to the global supply chain. NTU is a strong supporter of full and immediate expensing for structures, but we understand that some Democrats have opposed this proposal. Alternatives that are still pro-growth but reduce federal tax revenues less include neutral cost recovery (NCR) for structures and correcting the Tax Cuts and Jobs Act’s mistreatment of research and development costs.
Redesign Medicare Part D, including an out-of-pocket cap: NTU believes that perhaps the single health policy proposal with the most bipartisan momentum in 2020 is Medicare Part D redesign paired with an out-of-pocket cap. This would protect millions of seniors from exorbitant drug costs in the Medicare program, simplify the benefit design for patients, providers, CMS, plans, and manufacturers, and reduce taxpayer liability for drug costs beyond the catastrophic threshold. CBO also estimates it could save taxpayers tens of billions of dollars over the next decade. This was a centerpiece of the prescription drug legislation proposed by Senate Finance Committee Chairman Chuck Grassley (R-IA) and Ranking Member Ron Wyden (D-OR).
Enact a contract-based solution to surprise medical bills: As mentioned above, NTU supports a contract-based solution to the surprise medical billing problem, which would merely require that a provider who’s currently practicing at a facility be under contract to either 1) solely receive payment from the facility they practice at, or 2) receive payment from the same insurers as the facility contracts with. This would preserve some level of provider choice in contract negotiations while protecting patients from balance bills in most scenarios. The contract-based solution would accomplish all of this without establishing a new, complex government regime for setting prices or mediating disputes.
Take several steps to stabilize Medicare and Medicaid for the long term: Medicare is in trouble, with the Hospital Insurance (HI) trust fund projected to become insolvent in 2026. Medicaid appears to be on firmer financial footing, but surging enrollment under the ACA’s Medicaid expansion, the COVID-19 budget crunch, and long-running state practices threaten both Medicaid patients and the federal and state taxpayers who support the program. Earlier this year, NTU Foundation and U.S. Public Interest Research Group (PIRG) Education Fund identified three changes to the Medicare program that could collectively save taxpayers $167.5 billion over the next decade: 1) modify how risk scores are constructed ($67.2 billion), 2) provide authority to expand competitive bidding for certain durable medical equipment ($6.1 billion), and 3) reduce quality bonus payments to Medicare Advantage plans by eliminating Medicare Advantage benchmark increases that are tied to quality scores ($94.2 billion). Additional policy alternatives lawmakers should consider, with potential for bipartisan support, include: 1) eliminating the safe-harbor threshold for states’ Medicaid provider taxes ($344 billion in 10-year savings), 2) using a 50 percent FMAP for all Medicaid administrative expenses ($55 billion), 3) establishing uniform cost-sharing in Medicare Parts A and B ($44 billion), and 4) freezing income thresholds for income-related premiums in Medicare Parts B and D ($40 billion). The above seven policy options collectively save taxpayers $650 billion over 10 years.
In short, parts of both party agendas lack key details that will be crucial for the tens of millions of Americans with private health coverage and the taxpayers who support federal health programs. With the cost of health care rising, proposals to expand the federal government’s role in coverage and care demand detailed answers to tough questions from taxpayers. And while both platforms feature some laudable goals, such as ending surprise medical billing, a goal is not a policy proposal. Fortunately, months remain between now and Election Day, and candidates still have time to make a forceful and detailed case to voters.